Surgery is the cornerstone of treatment, and treatment depends greatly upon whether the cancer has invaded the muscle layer or not. Approximately 80% of bladder cancers are non-muscle-invasive bladder cancers and can be treated by transurethral resection of the bladder tumor (TURBT). Bladder cancers are resected and the bladder is often preserved. However, if the cancer has spread to the muscle layer, a radical cystectomy, or complete removal of the bladder, is usually performed.
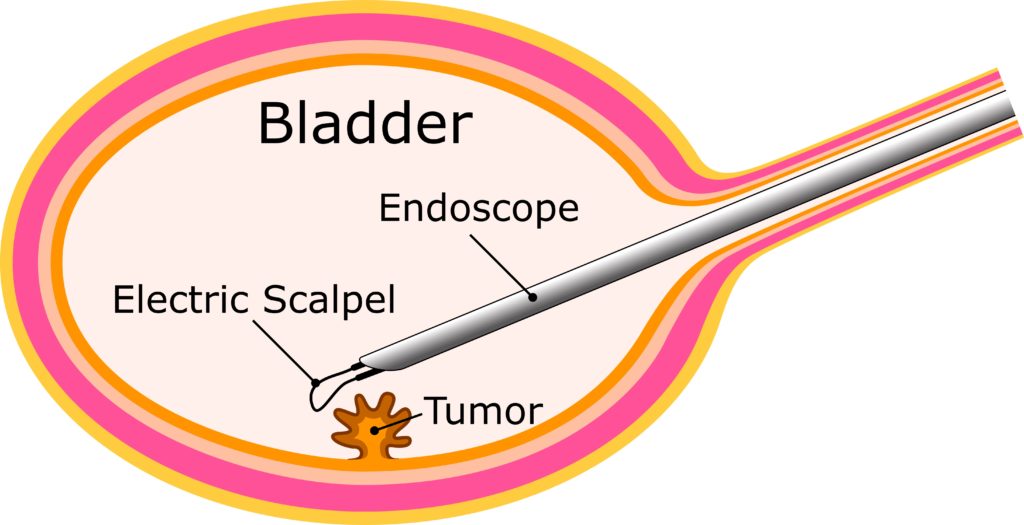
Endoscopic resection of bladder cancer, or TURBT, is a procedure whereby an endoscope is inserted through the urethra and the cancer is removed using a loop-shaped electric scalpel while observing the inside of the bladder (Fig. 3).
Non-muscle-invasive bladder cancers frequently occur at multiple sites in the bladder. Small lesions spread around the papillary carcinoma and the superficial flat cancers look normal and are hard to detect. The bladder can be preserved by TURBT, but some non-muscle-invasive bladder cancers are highly malignant, have a high rate of recurrence, and advance to more serious stages. The main cause of recurrence is considered to be the fact that small or flat cancers might not be detected by ordinary endoscopy and are easily overlooked. In order to reduce the risk of recurrence, it is important to improve the quality of TURBT so that cancers that are difficult to observe by appearance can be reliably detected, and residual cancer reduced (edited by the Japanese Urological Society Bladder Cancer Clinical Practice Guidelines 2019).
After resection of the bladder cancer, a pathological diagnosis is performed to determine the degree of malignancy and the depth of the cancer lesion. When the pathological diagnosis indicates a high risk of recurrence, chemotherapeutic agents or attenuated Mycobacterium tuberculosis (BCG) may be injected into the bladder. BCG is a vaccine against tuberculosis and is considered to boost the immune response and act on cancer cells. Also, in consideration of the risk of recurrence, a cystoscopy must be performed regularly after surgery (three months after initial treatment, followed by at intervals according to the risk). If cancer returns, additional TURBT will be performed, and the cancer may progress gradually over the course of recurrence. After recurrence, if the cancer reaches its worst stage, the bladder may have to be removed.
(Supervised by Dr. Yoshihiko Hirao, Director Emeritus, Osaka Gyoumeikan Hospital, Professor Emeritus, Nara Medical University)